Developing the right treatment for long COVID depends on figuring out what’s causing it. Stanford Medicine researchers are bent on learning more about the people who have it to find out.
March 8, 2023 - By Bruce Goldman
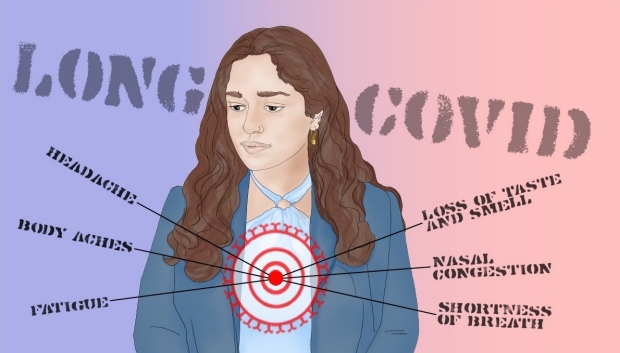
Stanford researchers are studying causes of and treatments for long COVID.
Linda Amoruso
Time heals many wounds. But not all of them.
Three years ago, on March 11, 2020, the World Health Organization officially bestowed pandemic status on COVID-19. Now, much of the fear that accompanied that declaration has subsided. We’ve turned the page on the virus, some have said.
Plenty of people still get COVID-19, and some people still get very sick from it. But fewer people are ending up in the hospital or dying at the hands of SARS-CoV-2, the virus that causes it. A variety of factors are responsible: herd immunity from vaccination or previous infections, new drugs, better medical techniques, more experienced health care workers, and a likely mellowing of lethality in now-dominant viral strains that have opted to trade in virulence for contagiousness.
Around half of the people who get infected by SARS-CoV-2 are asymptomatic — they don’t even know they had it.
But some infected people’s symptoms persist for months, or arise well after the acute case appears to have cleared up. The technical term for this syndrome is “post-acute sequelae of COVID,” or PASC, but even doctors and researchers refer to it as long COVID. And it’s got the medical community stumped.
The empty long-COVID toolbox
“Long COVID is a vitally important area of medicine,” said Linda Geng, MD, PhD, a clinical assistant professor of primary care and population health. Geng and Hector Bonilla, MD, a clinical associate professor of infectious diseases, are the co-directors of Stanford Health Care’s Post-Acute COVID-19 Syndrome Clinic, better known as the Stanford long-COVID clinic.
Linda Geng
“We have great tools in our toolbox for acute COVID,” Geng said. “We have no tools for long COVID.”
As COVID-19’s acute manifestations come under increasing control, a growing share of the disease’s medical and economic burdens is attributable to the still-climbing ranks of long-COVID patients.
“In 2020, we weren’t thinking about long COVID. We were worried about patients dying in the hospital, not brain fog or fatigue,” said Upinder Singh, MD, a professor and chief of infectious disease and geographical medicine, and a professor of microbiology and immunology. “Now we’re all emerging from the pandemic. Life is returning to normal. People are visiting family, going to parties. But long-COVID patients are getting left behind.”
So many questions
Stanford School of Medicine researchers are delving into the study and, they hope, conquest of this virally induced health hangover. Two research studies underway are aimed at defining long COVID’s characteristics, identifying its causes and testing therapeutic interventions that might treat it or prevent it.
The first big question the researchers are addressing: What, exactly, is long COVID?
Right now, the answer depends on who you ask. Long-COVID patients might exhibit any of 200 or more different symptoms of varying severity and duration. Symptoms can wax and wane, can emerge months after infection subsides, and might resemble those of a number of other conditions.
“The problem is, we don’t have a diagnostic biomarker for long COVID. We have to do more cumbersome clinical testing to exclude other causes of these symptoms,” Geng said.
Next question: How many people get long COVID?
Given its murky definition, it’s hard to tell who has it and who just thinks they do. Estimates range from 5% to 30% of all those who’ve been infected by SARS-CoV-2.
“Until you have a decent definition, there’s no way to put a number on it,” said PJ Utz, MD, a professor of immunology and rheumatology.
There’s no such thing as a typical long-COVID patient. One person can have a dozen symptoms, ranging from sleep disorders to autonomic-nervous-system dysfunction to headaches.
“This isn’t a case where you go into the doctor’s office with brain fog, a racing heart, lightheadedness, profound fatigue and dizziness and say, ‘Hey, can you test me for long COVID?’” Utz said. That test doesn’t exist yet.
How long can a person’s COVID’s symptoms persist? Only time will tell. It hasn’t been around long enough for anybody to know.

Upinder Singh
Who gets it? “In our clinic, about two-thirds of our patients are women,” Geng said. There are indications that newer strains impose a lower risk of patients ending up with long COVID. Some evidence suggests that the severity of initial symptoms is predictive and that vaccination is protective. But even people who initially had a mild case can get long COVID; vaccinated people, too, have some risk.
“The only guarantee is not getting COVID,” Geng said.
Six of long COVID’s most common symptoms are fatigue, cognitive difficulties (“brain fog”), body aches, shortness of breath, cardiovascular symptoms such as palpitations, and gastrointestinal problems. Having any of these symptoms, more than one month after testing positive for COVID-19, earns you a long-COVID diagnosis, according to the National Institutes of Health.
It could also get you into a clinical trial. Stanford Medicine is one of 15 designated sites for a set of upcoming large government-funded clinical trials focused on long COVID. Plus, Stanford School of Medicine scientists are conducting a solo, single-site clinical trial to see if they can kick long COVID to the curb.
Both trials are recruiting participants.
The “right treatment” for long COVID depends on what’s causing it. “We’re trying to understand underlying mechanisms and biology,” Utz said.
One theory holds that the virus is lingering in reservoirs in the body that the immune system doesn’t easily reach. The virus can either mount an active comeback or leave enough residual viral material floating around (or stuck to cell surfaces) to keep the immune system revved up to the point of exhaustion, rendering the patient vulnerable to other infections.
Another theory is that during acute COVID, the immune system is so busy fighting off SARS-CoV2 that it can’t suppress the resurgence of quiescent microbial invaders: for example, Epstein-Barr virus, which causes mononucleosis. Viruses such as Epstein-Barr hide out inside a healthy person’s organs, waiting to emerge when the beleaguered immune system lets its guard down.
Long COVID could also reflect residual effects of damage the initial infection inflicted on a person’s lungs, brain or you name it. SARS-CoV-2 can damage the cells that line all of our blood vessels, leading to ill effects in practically any organ. This could also spur the formation of traveling microscopic blood clots that, in principle, can lodge anywhere in the body.
Another possibility, with evidence to back it up: The virus tricks the body into attacking its own tissue or secretions. Utz has found meaningful increases in blood levels of autoantibodies among people who’ve contracted severe COVID-19. Antibodies are proteins certain immune cells produce as weapons to disable invading pathogens. Autoantibodies are antibodies that target our own innocent tissues or signaling substances immune cells secrete to communicate with one another — a possible step toward autoimmunity.
To the rescue
In the first week of December 2020, Utz attended a two-day Zoom workshop on long COVID convened by Anthony Fauci, MD, then the head of the National Institute for Allergy and Infectious Diseases. There, several patients described what they were going through.
PJ Utz
“It was a real eye-opener,” Utz said. “When you hear about otherwise high-functioning people like this who are so sick they can’t get out of bed in the morning, you know something is wrong. They’re not making it up.”
That workshop laid the groundwork for a $1.125 billion NIH-funded research initiative that’s dedicated to studying and ameliorating long COVID. The initiative is called RECOVER (for REsearching COVid to Enhance Recovery). Researchers across the country will enroll more than 17,000 adult participants as well as thousands of children in the study.
Stanford Medicine, one of the first of the 15 research sites to get off the starting block, has enrolled nearly 1,000 participants — long-COVID patients as well as people who’ve never had COVID, as controls — and is still recruiting. (Get more details here or email treatcovid@stanford.edu.) The investigators will monitor participants for four years. They’ll identify differences between people who have long COVID and those who don’t, and they’ll watch what happens to those who do. As part of that, they will examine participants’ blood and stool samples for molecular signatures, or biomarkers, that correlate with symptom severity. Once those are found, they’ll look for treatments that bring long-COVID patients’ biomarkers back to healthy baseline levels.
Stanford Medicine is also running a clinical trial, designated STOP-PASC. (STOP stands for Selective Trial Of Paxlovid; PASC is for Post-Acute Sequelae of COVID.)
“We’re testing an orally available antiviral medication, Paxlovid, to see if the notion of a viral reservoir holds up and if we can help long-COVID sufferers feel better,” Geng said.
Paxlovid, developed by Pfizer, received an emergency use authorization for high-risk people with mild to moderate acute COVID-19 after a five-day course of the drug safely reduced hospitalizations and deaths by nearly 90% compared with placebo in large clinical trials.
STOP-PASC researchers are shooting for 200 participants and actively recruiting people who’ve had moderate to severe long-COVID symptoms for more than three months. Participants receive Paxlovid or a placebo for 15 days, then undergo monitoring for 15 weeks. The trial is randomized and double-blinded. (Get more information here or email treatcovid@stanford.edu). Apply for participation in the trial via this link.)
Some participants will also be given a smartwatch that will track their heart rates, physical activity, sleep patterns and oxygen saturation.
Utz’s lab and others will analyze participants’ blood and stool samples, searching for substances or constellations of them that could serve as biomarkers of long COVID, and see how they change upon administration of the drug versus the placebo.
“There are a lot people out there with long COVID who are clearly suffering and are worried that people think they’re crazy,” Utz said. “We’re doing this study because we’re convinced that long COVID is a real syndrome that requires us to better understand what’s causing it and come up with ways to treat people who have it.”
-
 Bruce GoldmanBruce Goldman is a senior science writer in the Office of Communications. Email him at goldmanb@stanford.edu.
Bruce GoldmanBruce Goldman is a senior science writer in the Office of Communications. Email him at goldmanb@stanford.edu.
About Stanford Medicine
Stanford Medicine is an integrated academic health system comprising the Stanford School of Medicine and adult and pediatric health care delivery systems. Together, they harness the full potential of biomedicine through collaborative research, education and clinical care for patients. For more information, please visit med.stanford.edu.