Stanford Minimally Invasive Thoracic Surgery
(SMITS) Center
The Stanford Center for Minimally Invasive Thoracic Surgery (SMITS), co-directed by Drs. Mark Berry and Joseph Shrager, was founded in 2014 to recognize Stanford's position among the leading thoracic surgery centers in the United States in experience and expertise in minimally invasive approaches to chest diseases.
Our surgeons were early adopters of minimally invasive techniques as it became clear that they have substantial benefits to patients when used appropriately. Our surgical outcomes have most recently been ranked within the top 6% of programs in the country by the Society of Thoracic Surgeons General Thoracic Surgery Database, earning us the highest, 3-star rating for our pulmonary lobectomy results. This database tracks outcomes primarily for specialized, large, academic medical center thoracic surgery practices. In other words, our results fall within the top 7% of a very elite group. We have also been deemed a "high performing hospital" in lung cancer surgery by U.S. News and World Report.
Before the development of minimally invasive surgical techniques in recent decades, patients who needed thoracic surgery to treat conditions such as lung or esophageal cancer required open approaches, which are more challenging for the body to heal. In a traditional thoracotomy, surgeons make a long incision down the patient's side and spread the ribs. In a median sternotomy, surgeons divide and spread the breast bone. In a laparotomy, they make a long incision over the abdomen and retract the muscles of the abdominal wall.
These surgical approaches made possible many life-saving thoracic surgery procedures, which surgeons have performed precisely and safely for many years. But they require a prolonged recovery period during which patients must restrict physical activity to allow the incisions and other surgical trauma to heal. Patients who are elderly, frail, or have other significant medical problems, such as heart or lung disease, are sometimes simply not well enough to undergo these procedures safely.
With the rise of advanced video technology and robotic surgical tools, surgeons can now perform thoracic surgical procedures using small incisions through which long, thin instruments are inserted. These minimally invasive thoracic surgical procedures are often referred to as thoracoscopy, video-assisted thoracic surgery (VATS), or robotic thoracic surgery. They allow surgeons to perform the same procedures inside the patient's body with less trauma to the chest wall or abdominal wall.
The advantages of these minimally invasive approaches are:
Smaller incisions with lower risk of infection
Shorter hospital stays
Less external trauma, which may mean less pain and faster return to normal activities
Less tissue damage, which may reduce the chances of post-surgical complications such as pneumonia
Less internal scar tissue, which can reduce the complexity of any future surgeries the patient may need
Improved ability to tolerate other cancer treatments, such as chemotherapy, that optimize the patient's chance of becoming cancer-free.
Stanford uses minimally invasive surgical techniques whenever possible.
In 2015, approximately 70% of lung surgeries at Stanford were performed with a VATS minimally invasive technique.
Patients with esophageal cancer often get minimally invasive esophagectomy (MIE) rather than laparotomy or thoracotomy. In 2015, more than 80% of esophageal surgeries at Stanford utilized minimally invasive surgical techniques.
To avoid median sternotomy, Stanford doctors often use VATS, robotic surgery, or laparoscopy to treat conditions such as paralyzed diaphragms, hiatal hernias, reflux disease, achalasia or other conditions of the mediastinum.
{kind=link}
Stanford thoracic surgeons have specialized training and experience with all minimally invasive thoracic surgical procedures, as well as with traditional open procedures. They have published many scientific studies critically investigating the performance and effectiveness of minimally invasive approaches. They also have extensive experience in teaching other surgeons these techniques in courses at the local, national, and international level.
We continue to collect and review results data regularly, and critically, in order to assure the highest level of quality control and patient safety and satisfaction.
We consider all patients for minimally invasive approaches. However, minimally invasive thoracic surgical procedures are not necessarily appropriate for all patients. Previous surgery or treatment or tumor size or location can make minimally invasive techniques inappropriate for some patients. They may increase the risk of potentially serious intra-operative bleeding or other complications or compromise the surgeon's ability to completely remove the tumor.
The extensive training and experience that Stanford thoracic surgeons have with both open and minimally surgery allow them to select the most appropriate procedure for every individual patient. Patients can rely on the highest quality of care whichever procedure they ultimately undergo.
If you would like to make an appointment to see one of our surgeons, please call (650) 498-6000 and ask for the Thoracic Surgery new patient coordinator, or call (650) 721-2086.
Our Thoracic Team
Joseph Shrager, MD
Division Chief, Professor, Co-Director Thoracic Oncology Clinical Care Program
Co-director SMITS

Mark Berry, MD
Mylavarapu Rogers Professor
Co-director SMITS

Leah Backhus, MD, MPH, FACS
Professor
Natalie Lui, MD
Assistant Professor

Douglas Liou, MD
Clinical Associate Professor
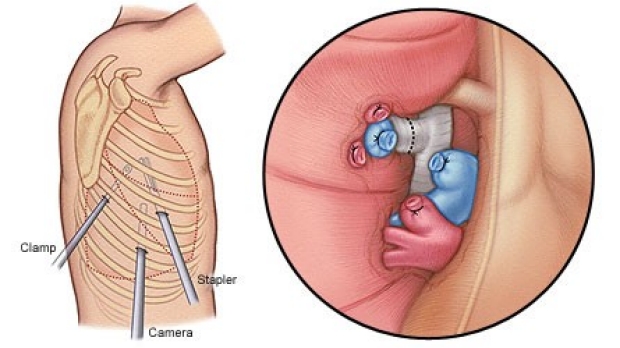
VATS Lobectomy
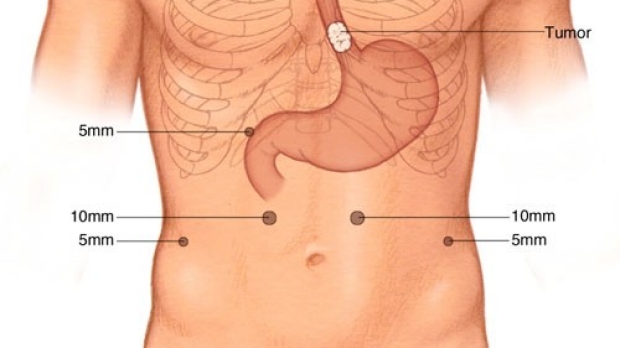
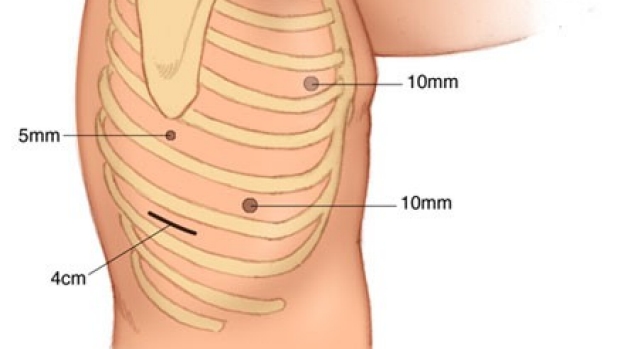
Laparoscopic incisions for Minimally Invasive Ivor Lewis Esophagectomy
The right VATS incisions that are used to mobilize the esophagus.
The Division of Thoracic Surgery in the Department of Cardiothoracic Surgery at the Stanford School of Medicine is located in the San Francisco Bay Area in northern California. For more information about our services, please contact Donna Yoshida at (650) 721-2086 or Cliff David at (650) 721-6400. For new patient Thoracic Surgery Clinic Scheduling, please call (650) 498-6000.